Diary of an Oral Health Educator - Week One - Motivating change in children
Diary of an Oral Health Educator - Week One - Motivating change in children
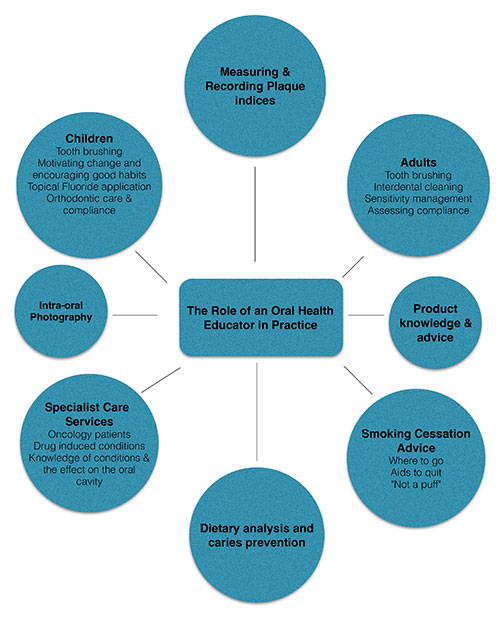
The role of an oral health educator can be very rewarding, not only on a personal level, but to the patient and also to a dental business. However, it can also be sadly underestimated or undervalued.
I am fortunate enough to work in a practice that values prevention and education for all, and that as such provides complementary access to an oral health educator for all patients paying membership, and for those not on our membership scheme on the payment of a small one-off fee of £10.
This week I reviewed a young girl (7 years old) who has required several appointments to motivate change. She was referred to me by the dentist for having poor oral hygiene, hyper-plastic deciduous molars and first molars, and for being in need of restoratives. The dentist had asked me to provide advice on tooth brushing and diet, as well as a programme of topical fluoride application.
On the first appointment I always start by introducing myself and attempting to discover what a child's knowledge or understanding is of why it is important to brush your teeth. I get a variety of answers from ’to make them shiny’ or ’so they don't go rotten or fall out’ to ‘to get rid of plaque and food’. The level of response is, of course, dependent on the age of the child.
On this occasion, two siblings attended with their nanny (au pair) but not the parents.
I gave both girls GC Triplaque solution, which I find very effective when treating children and the accompanying adult as it shows plaque deposits, ageing from less than 24 hours up to more than 48 hours, and potentially acidic plaque. It is normally at this point that I have their full attention.
It's often useful at this stage to take intra-oral pictures which can be stored in the patient records and easily accessed and referred back to at future appointments to compare progress.
We worked with both a manual toothbrush and an electric toothbrush to find out which brush the girls could cope with best. As an oral health educator, I do always encourage the use of an electric toothbrush but of course they are only more effective if used correctly. I have found that some children perform better with a good old-fashioned manual brush. I ask that children bring their own brush to the appointment as well, to see what they are provided with at home. Very often problems with poor brushing can be identified easily by a flat splayed out brush or a brush that would give a thoroughbred horse good oral hygiene but that is clearly too big for a small developing mouth.
There are occasions when I really need to work very closely with a family to motivate change and to create the necessary focus.
My first obstacle in this situation was the nanny. I asked her at the initial appointment to take photos on her phone so that she could report back to the parents and impress on them the help that these two young girls required at home. It didn't happen, so that when mum actually attended with the girls her reaction was a bag of very mixed emotions.
Now we could get to work. Once the mom was aware, it meant that the morning and bedtime routines for brushing were going to be more supervised and assisted. We needed to stabilise the little girl’s oral hygiene and get her to a standard where she could then cope with brushing unaided but supervised.
It is really important when dealing with children that you remain positive, giving praise and encouragement at every opportunity. By motivating change, we are encouraging good habits for later in life, but it can be very hard when improvement doesn't happen. In this case there were set backs where the focus and encouragement was there with the parents, but they admittedly became complacent.
Mum did confide to me that she had readdressed her life, cutting down her working hours and reducing the amount of time that the children spent with a nanny. The two girls are now showing huge improvement in their oral hygiene and mum seems to be more relaxed and in control. The younger of the two girls will continue on a rolling three monthly programme to check her oral hygiene and for the topical application of fluoride to her hyperplastic enamel.
As I said at the beginning, the role of an oral health educator can be underestimated. It is not just about teaching someone how to use a toothbrush correctly. They really do have to take a holistic approach to care; in this case the ‘whole body’ is the family. There are so many other benefits to your patients for having a practice-based oral health educator. For the oral health educator there is so much job satisfaction from engaging with patients, and from helping to bring about important changes in their lives and consequent self-developmet.